



















In our quest to understand bloodborne odor problems as best we can, this is another post about the xenobiotic metabolizing enzymes, also known as the drug metabolizing enzymes or biotransformation enzymes. This is the group of enzymes largely responsible for dealing with external foreign compounds, and altering them into something the body knows what to do with - in the case of toxins, turning them into water soluble non-toxic compounds. These enzymes also catalyze metabolic processes with internal compounds. They deal with compounds of similar structures.
At the moment, these seem like a natural parameter for looking for a 'metabolic' culprit(s) in fecal body odor and other 'non-specific' metabolic body odors. Other enzymes seem to be quite specific for certain substrates, and perhaps a sufferer will have a certain smell only, such as 'sweaty feet syndrome' with isovaleric acidemia. But at the moment this is speculation. We don't want to rule anything out, but this group of cell enzymes seem the first point of enquiry.
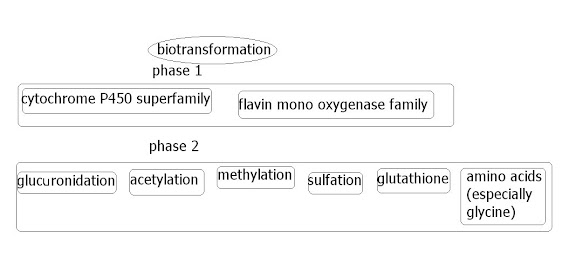
Xenobiotic enzymes are mostly situated in the liver cells, but are also present in cells anywhere the body, as the evolutionary process over the generations has deemed sensible. (e.g. the small intestine. Grapefruit juice can greatly inhibit CYP3A4 activity in the small intestine, but seemingly not the CYP3A4 in the liver). Phase1 seems to be enzymes that catelyses oxidation, reduction or hydrolyze reactions. Phase2 enzymes are known as 'conjugating enzymes'; they add a molecule to a compound to make it neutral and water soluble. For instance, in sulfation, a sulfur molecule is added.
The phase1/phase2 approach may not be commonly used, yet possibly still taught to medical students. Currently FMO3 is likely not given as much importance compared to CYP450 as is noted in the article, Flavin mono-oxygenase (FMO)--the 'other' oxidase, by an FMO3 expert (Mitchell SC in London). Some may see their point, since most with TMAU seem to be 'fine' apart from the smell. But other health problems may turn out to be associated. Such as chronic fatigue, or aggravation to other medical conditions such as neurological conditions (learning disabilities, anxiety, epilepsy, fibromyalgia, auto-immune diseases, etc.) . Only time will tell.
Medical students are likely taught that any 'deficiency' in a xenobiotic metabolizing enzyme is likely to do with a phase 1 enzyme, and that phase 2 are rarely deficient, but 5% (or more) of the population are estimated to have a weak 'glucuronidation' enzyme. This is regarded as usually 'benign' but testimonies on the problem seem to indicate differently. Often the sufferer will easily develop jaundiced, since this enzyme is greatly responsible for detoxing bilirubin. It's known as Gilberts Syndrome.
Hopefully the CYP450 article below will add to understanding these enzymes.
http://www.anaesthetist.com/physiol/basics/metabol/cyp/Findex.htm#cyp.htm








0 comments: